Acidic fibroblast growth factor (aFGF), also known as FGF-1, ECGF and HBGF-1, is a non-glycosylated heparin binding growth factor and member of the FGF family of mitogenic peptides. It is involved in several important physiological and pathological processes, such as embryonic development, morphogenesis, angiogenesis, wound healing and atheromatosis (1). aFGF is expressed in the brain, kidney, retina, smooth muscle cells, bone matrix, osteoblasts, astrocytes and endothelial cells. It is the only member of the FGF family that binds with high affinity to all four FGF receptors (2). aFGF binds to cell surface receptors with high affinity with the prerequisite association with heparin sulfate. This ligation subsequently initiates receptor dimerization, transphosphorylation, as well as internalization of receptor/FGF complexes, and thus aFGF is translocated across cellular membranes and transported to the nucleus. The FGF pathway regulates primitive hematopoiesis by modulating transcription factors such as Gata1 expression level and activity (3). aFGF has been implicated in an autocrine system by which calcium regulates parathyroid cell growth. It has been demonstrated that the expression of aFGF is highest during the late stages of hepatic morphogenesis in newborn rats as well as during hepatic differentiation in adult liver. The intravenous application of aFGF has shown that the factor promotes the regeneration of the endothelium following arterial intravascular injuries (4). Overexpression of aFGF in pancreatic cancers has been found to be associated with a more advanced tumor stage. Recent studies have also demonstrated that chimeric toxins composed of aFGF fused to mutant forms of Pseudomonas exotoxin, are cytotoxic to a variety of tumor cell lines with FGF receptors (5).
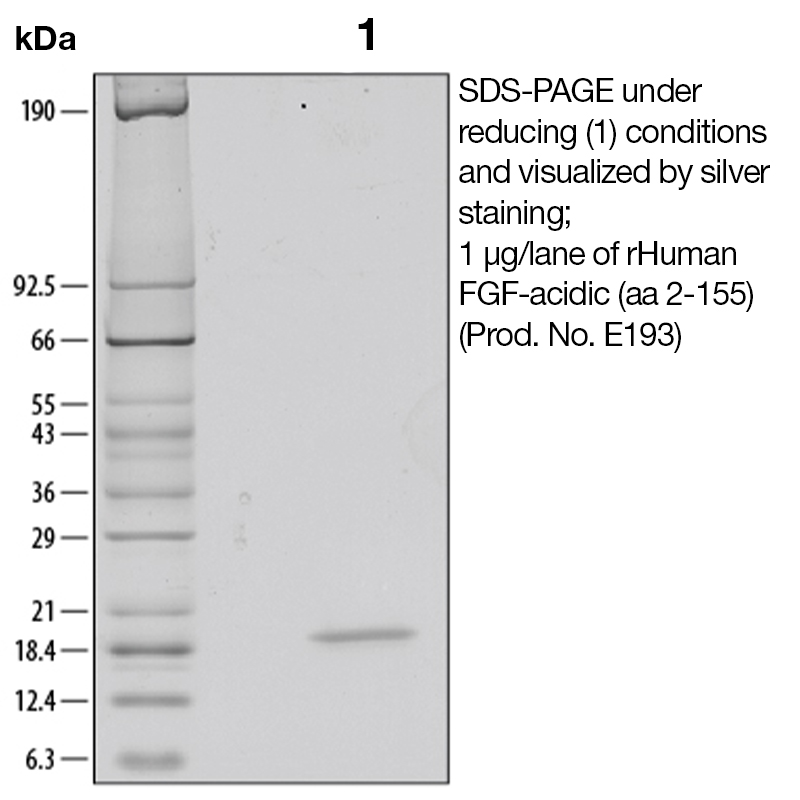
The predicted molecular weight of Recombinant Human β-ECGF is Mr 17 kDa.
Predicted Molecular Mass
17
Formulation
This recombinant protein was lyophilized from a 0.2 μm filtered solution in MOPS, sodium sulphate (Na2SO4), ethylenediaminetetraacetic acid (EDTA), and dithiothreitol (DTT).
Storage and Stability
This lyophilized protein is stable for six to twelve months when stored desiccated at -20°C to -70°C. After aseptic reconstitution, this protein may be stored at 2°C to 8°C for one month or at -20°C to -70°C in a manual defrost freezer. Avoid Repeated Freeze Thaw Cycles. See Product Insert for exact lot specific storage instructions.
Powered by AI: AI is experimental and still learning how to provide the best assistance. It may occasionally generate incorrect or incomplete responses. Please do not rely solely on its recommendations when making purchasing decisions or designing experiments.
Recombinant Human FGF-Acidic (aa 2-155) is widely used in research due to its potent ability to stimulate cell proliferation, support tissue regeneration, and promote angiogenesis, making it valuable for studies in developmental biology, wound healing, stem cell culture, and disease modeling.
Key scientific reasons to use this protein in your research applications include:
Broad Mitogenic Activity: FGF1 (acidic FGF) stimulates proliferation of cells from all germ layers—mesodermal, neuroectodermal, ectodermal, and endodermal origins—making it suitable for diverse cell culture systems and tissue engineering.
Role in Development and Regeneration: It is critical for embryonic development, tissue repair, and regeneration, and is often used to model these processes in vitro and in vivo.
Angiogenesis: FGF1 is a potent angiogenic factor, promoting endothelial cell proliferation and migration, which is essential for vascular biology studies and regenerative medicine.
Wound Healing: Recombinant FGF1 has been shown to accelerate wound healing and tissue repair, both in animal models and clinical settings, making it a tool for studying mechanisms of tissue regeneration and for developing therapeutic approaches.
Stem Cell Applications: FGF1 supports the maintenance and proliferation of stem cells, and is used in protocols for differentiation and expansion of pluripotent and multipotent stem cells.
Disease Modeling: Its involvement in processes such as tumor growth, neurogenesis, and metabolic regulation makes it relevant for cancer research, neuroscience, and metabolic disease studies.
Technical considerations:
The aa 2-155 construct represents the mature, bioactive form of human FGF1, lacking the N-terminal methionine, which may improve solubility and biological activity in recombinant systems.
Recombinant FGF1 is typically produced in E. coli and supplied as a lyophilized protein, often with carrier proteins to enhance stability.
FGF1 requires heparan sulfate or heparin for optimal receptor binding and activity, so supplementation in cell culture may be necessary.
Summary of applications:
Cell proliferation assays
Angiogenesis and vascular biology studies
Wound healing and tissue regeneration models
Stem cell maintenance and differentiation
Cancer biology and tumor microenvironment research
Neurogenesis and neuronal survival studies
Using recombinant human FGF-Acidic (aa 2-155) provides a well-characterized, consistent, and bioactive growth factor for these applications, facilitating reproducible and physiologically relevant experimental outcomes.
You can use Recombinant Human FGF-Acidic (aa 2-155) as a standard for quantification or calibration in your ELISA assays, provided it is of high purity and its concentration is accurately determined. However, there are important considerations to ensure reliable and valid results.
Key considerations:
Purity and Characterization: The recombinant FGF-Acidic (aa 2-155) protein you referenced is reported to be >97% pure and derived from E. coli, which is suitable for use as a standard in ELISA if the protein is properly folded and free of significant contaminants.
Standard Curve Preparation: For quantitative ELISA, standards should be prepared using a purified or well-characterized recombinant protein. The concentration of your standard must be accurately known, and the protein should be reconstituted and diluted according to best practices to ensure consistency and reproducibility.
Epitope Recognition: The recombinant standard must include the epitope(s) recognized by the capture and detection antibodies in your ELISA. The aa 2-155 construct covers the full mature FGF1 sequence, which is typically recognized by commercial ELISA kits for FGF1/FGF-acidic.
Matrix Effects: If your samples are in a complex matrix (e.g., serum, plasma), prepare your standard curve in the same matrix or use appropriate diluents to minimize matrix effects and ensure accurate quantification.
Carrier Protein: Some recombinant FGF1 proteins are supplied with carrier proteins (e.g., BSA) to enhance stability. If your ELISA is sensitive to carrier proteins, use a carrier-free preparation or ensure the carrier is compatible with your assay.
Best Practices:
Confirm that your ELISA kit or in-house assay is validated for use with recombinant FGF1 standards of the same sequence and source (E. coli-derived, aa 2-155).
Follow the manufacturer’s instructions for reconstitution and dilution of the standard protein.
Validate the standard curve for linearity and parallelism with your sample matrix to ensure accurate quantification.
Summary Table: Use of Recombinant FGF-Acidic (aa 2-155) as ELISA Standard
Requirement
Met by Recombinant FGF-Acidic (aa 2-155)?
Notes
High purity
Yes (>97%)
Confirm with your batch
Full mature sequence
Yes (aa 2-155)
Covers typical ELISA epitopes
Accurate concentration
User must verify
Use precise quantification methods
Carrier protein compatibility
Depends on preparation
Use carrier-free if BSA interferes
ELISA antibody compatibility
Likely, but must confirm
Check kit/antibody datasheets for epitope coverage
If all these criteria are met, Recombinant Human FGF-Acidic (aa 2-155) is appropriate for use as a standard in ELISA quantification. Always validate the standard curve in your specific assay context.
Recombinant Human FGF-Acidic (FGF1, aa 2-155) has been validated for several applications in published research, primarily centered around its roles in cell proliferation, tissue regeneration, and signaling pathways. Key applications supported by the literature include:
Cell Proliferation and Bioassay: FGF1 is widely used as a mitogen to stimulate the proliferation of various cell types, including mesoderm-, neuroectoderm-, ectoderm-, and endoderm-derived cells. It is commonly applied in bioassays to assess mitogenic activity and cell growth (e.g., in fibroblasts, endothelial cells, and stem cells) [1, 2, 3, 4, 8, 10, 13].
Wound Healing and Tissue Regeneration: FGF1 has been shown to promote wound healing and tissue regeneration, particularly in models of skin wound repair and endothelial regeneration following vascular injury [3, 5, 12].
Angiogenesis: FGF1 is involved in the formation of new blood vessels and has been used in studies investigating angiogenesis and vascular development [1, 3, 4, 12].
Development and Organogenesis: FGF1 plays a role in embryonic development and organogenesis, and has been used in studies of developmental biology, including limb and nervous system development [1, 8, 12].
Neuroprotection and Neuroregeneration: FGF1 has been shown to suppress apoptosis in neurons and promote neuroprotection, making it relevant for studies on nerve injury and neurodegenerative diseases .
Stem Cell Culture and Differentiation: FGF1 is used in the culture and differentiation of stem cells, including induced pluripotent stem cells (iPSCs) and embryonic stem cells, particularly in protocols for retinal differentiation and hepatocyte-like cell generation [2, 4].
Cancer Research: FGF1 has been implicated in tumor growth and progression, and is used in studies investigating the role of FGF signaling in cancer biology and as a potential therapeutic target [3, 12].
Metabolic and Cardiovascular Research: FGF1 has been shown to regulate cardiogenesis and adipose tissue remodeling, and has been used in studies on metabolic diseases and cardiovascular development .
These applications are supported by studies using recombinant human FGF1 (aa 2-155) in various experimental models, including cell culture, animal models, and bioassays.
To reconstitute and prepare Recombinant Human FGF-Acidic (aa 2-155) for cell culture experiments, dissolve the lyophilized protein at a concentration of 100 μg/mL in sterile PBS containing at least 0.1% human or bovine serum albumin (BSA). This carrier protein helps stabilize FGF-Acidic and prevents adsorption to surfaces.
Step-by-step protocol:
Centrifuge the vial briefly before opening to ensure all powder is at the bottom.
Add sterile PBS (pH 7.2–7.4) containing 0.1% BSA to achieve a final concentration of 100 μg/mL.
Gently mix by pipetting up and down or by gentle inversion; do not vortex or shake vigorously, as this may denature the protein.
Aliquot the solution into working volumes to avoid repeated freeze-thaw cycles.
Store aliquots at 2–8 °C for up to 1 month, or at –20 °C to –70 °C for up to 3 months under sterile conditions.
Further dilutions for cell culture:
Make additional dilutions in cell culture medium or buffer containing 0.1% BSA to maintain protein stability.
For functional assays, typical working concentrations range from 0.015–0.15 ng/mL (ED50 for cell proliferation), but optimal concentrations should be determined empirically for your cell type.
Additional notes:
Avoid repeated freeze-thaw cycles, as these can reduce protein activity.
If the protein was lyophilized from a buffer containing reducing agents (e.g., DTT, TCEP), ensure compatibility with your cell culture system.
If your protocol or supplier recommends a different buffer (e.g., 5 mM sodium phosphate, pH 7.6), follow those instructions for initial reconstitution.
Summary Table:
Step
Buffer/Conditions
Concentration
Storage
Reconstitution
PBS + 0.1% BSA (sterile)
100 μg/mL
2–8 °C (1 mo), –20 °C (3 mo)
Working dilution
Cell culture medium + 0.1% BSA
0.015–0.15 ng/mL (ED50)
Aliquoting
Avoid repeated freeze-thaw
As needed
This protocol ensures optimal stability and bioactivity of FGF-Acidic for cell culture applications.
References & Citations
1. Jaye, M. et al. (1986) Science 233:541 2. Otlewski, J. et al. (2009) Acta. Crystallogr. D. Biol. Crystallogr. 65:67 3. Nakazawa, F. et al. (2006) Blood. 108:3335 4. Bjornsson, TD. et al. (1991) Proc. Natl. Acad. Sci. (USA) 88:8651 5. Merwin, JR. et al. (1992) Cancer Res. 52:4995





 Products are for research use only. Not for use in diagnostic or therapeutic procedures.
Products are for research use only. Not for use in diagnostic or therapeutic procedures.