

Anti-Human CD68 (Clone KP1) – Purified No Carrier Protein


Anti-Human CD68 (Clone KP1) – Purified No Carrier Protein
Product No.: C920
Clone KP1 Target CD68 Formats AvailableView All Product Type Hybridoma Monoclonal Antibody Isotype Mouse IgG1 κ Applications B , EM , FC , ICC , ICFC , IHC , IHC FFPE , IP , WB |
Data
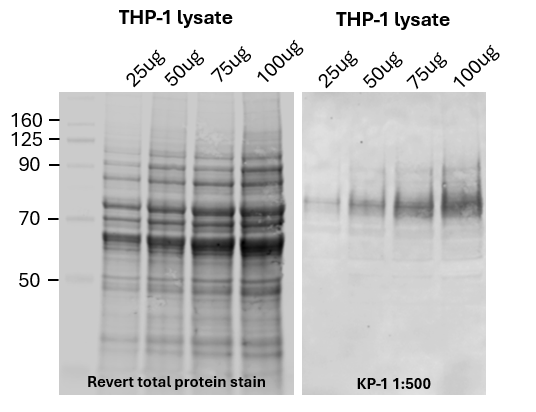 Western blot (right)
Western blot (right)Varying quantities of cell lysates were run on a 4-12% XT-Bis Tris gel in MES buffer.
Blot was incubated with primary antibody clone KP-1 (1:500) in PBS-T and goat anti-mouse IR-800 (LI-COR, 1:20,000) was used for detection on a LI-COR Odyssey.
*Data generously provided by Ryan Chen and Valentina Rangel-Angarita of the Dr. Stacy Malaker Lab at Yale University
Antibody DetailsProduct DetailsReactive Species Human Host Species Mouse Product Concentration ≥1.0 mg/ml Purity ≥90% monomer by analytical SEC and SDS-Page Formulation This monoclonal antibody is aseptically packaged and formulated in 0.01 M phosphate buffered saline (150 mM NaCl) PBS pH 7.2 - 7.4 with no carrier protein, potassium, calcium or preservatives added. Due to inherent biochemical properties of antibodies, certain products may be prone to precipitation over time. Precipitation may be removed by aseptic centrifugation and/or filtration. Product Preparation Purified antibodies are manufactured in an animal free facility using only in vitro protein free cell culture techniques and are purified by a multi-step process including the use of protein A or G to assure extremely low levels of endotoxins, leachable protein A or aggregates. Storage and Handling Functional grade preclinical antibodies may be stored sterile as received at 2-8°C for up to one month. For longer term storage, aseptically aliquot in working volumes without diluting and store at -70°C. Avoid Repeated Freeze Thaw Cycles. Country of Origin USA Applications and Recommended Usage? Quality Tested by Leinco FC5, 10, 12, WB4, 7, 10, Additional Applications Reported In Literature ? IHC5, 7, 8, 9, 10, 11, IHC FFPE10, IP1, 4, 10, 12, ICFC5, 7, ICC4, 12, Dot12, B12, EM2, Each investigator should determine their own optimal working dilution for specific applications. See directions on lot specific datasheets, as information may periodically change. DescriptionDescriptionSpecificity Anti-CD68 antibody (clone KP1) activity is directed against human CD68. Background CD68 is a heavily glycosylated type I transmembrane glycoprotein belonging to the lysosomal-associated membrane protein (LAMP) family and may play a role in endocytosis or lysosomal traffic and phagocytic activities1. CD68 localizes to endosome- or lysosome-like structures2. Additionally, LAMPS have been implicated in tumor cell metastasis and are over-expressed on the surface of metastatic compared with nonmetastatic cell lines3.
KP1 was originally used as a pan-monocytic/macrophage marker against CD68; however, CD68 is not a macrophage specific antigen and KP1 is known to stain neutrophils and other non-macrophage-like cells4,5,6,7,8. KP1 reacts against CD68 in a wide range of healthy4 and disease-associated (rheumatoid arthritis and osteoarthritis)5 tissues as well as a variety of neoplasms9, tumor cell lines7, and tumor-associated macrophages 8. KP1 detects a fixation-resistant epitope10 that is likely glycan-based1,9 which is shared by many cell types7. KP1 was developed by immunizing Balb/c mice against a lysosomal fraction of human lung 10. Hybridoma supernatants derived from spleen cells were screened on cryostat human lung and tonsil sections as well as paraffin wax sections of lung tissue fixed in formol saline. Antigen Distribution CD68 is found in the cytoplasm of monocytes/macrophages, fibroblasts, human peripheral blood lymphocytes, neutrophil primary and mast cell granules, large granular lymphocytes, basophils, basal epithelial cell layers, renal glomeruli, myeloid cells, endothelial cells, retinal epithelial cells, osteoblasts, fibroblast-like cells from bone marrow, and a wide-range of lymphoid neoplasms. CD68 is predominantly located in lysosomal membranes, with a small amount on the cell surface. Additionally, CD68 can be expressed in most hematopoietic cell lines by phorbol-induced differentiation; soluble CD68 can also be found in serum and urine. NCBI Gene Bank ID Research Area Immunology Leinco Antibody AdvisorPowered by AI: AI is experimental and still learning how to provide the best assistance. It may occasionally generate incorrect or incomplete responses. Please do not rely solely on its recommendations when making purchasing decisions or designing experiments. Clone KP1 is an anti-human CD68 monoclonal antibody with specific applications in in vivo mouse studies. Its primary use focuses on immunohistochemical staining of human macrophages or monocytes in xenograft models, where human cells are engrafted into mice, such as studies on humanized mice or tumor xenografts. Applications in Xenograft ModelsThe clone is particularly valuable for researchers working with mouse models that contain human cells. In these experimental settings, KP1 enables the identification and characterization of human macrophages and monocytes that have been introduced into the mouse system. This specificity for human CD68—a 110 kDa glycoprotein predominantly expressed on intracellular lysosomes of monocytes and macrophages—makes it an essential tool for distinguishing human immune cells from murine cells in mixed populations. Technical ConsiderationsFor in vivo mouse studies, clone KP1 is typically used in functional grade purified formats without carrier proteins, which ensures compatibility with the stringent requirements of in vivo research. The antibody recognizes human CD68 and shows cross-reactivity with primate and rat species, though its primary utility in mouse models remains focused on detecting human cells rather than mouse cells. The typical applications include immunohistology on paraffin-embedded tissues, immunofluorescence, flow cytometry, and western blotting of human cells within mouse tissues, allowing comprehensive analysis of human macrophage populations and their distribution in various experimental contexts. Other commonly used antibodies and proteins that appear alongside KP1 (anti-CD68) in the scientific literature serve to identify and distinguish various immune cell populations, particularly within the monocyte/macrophage lineage and related cell types. Monocyte/Macrophage MarkersThe most frequently paired antibodies include CD14, CD163, and CD11b, which are markers specifically used for identifying cells within the monocyte/macrophage lineage. These markers help researchers comprehensively characterize macrophage populations and distinguish between different activation states or subpopulations of these immune cells. Context-Dependent SelectionThe choice of antibody combinations used with KP1 is highly context-dependent and tailored to specific research needs. Scientists select these combinations based on several objectives: Distinguishing immune cell types - Different antibody panels help differentiate between macrophages and other immune cells present in tissues Diagnosing hematopoietic neoplasms - Specific marker combinations aid in identifying and classifying blood cell cancers Characterizing tissue environments - Antibody panels help analyze inflammation patterns and tumor microenvironments, particularly when studying tumor-associated macrophages The specific combinations chosen depend on whether researchers are working with normal tissues, diseased tissues (such as rheumatoid arthritis or osteoarthritis), various neoplasms, tumor cell lines, or specialized models like human tumor xenografts in mice. In xenograft studies, KP1 is particularly valuable because it specifically delineates the human myeloid compartment against the murine background, allowing precise identification of human-derived macrophages. Clone KP1 represents a significant monoclonal antibody in immunohistochemistry and macrophage research, with key findings spanning several decades of scientific investigation. This antibody has become a fundamental tool for identifying and studying cells of the monocyte/macrophage lineage in both normal and diseased tissues. Antibody Characteristics and SpecificityKP1 was developed by immunizing BALB/c mice against a lysosomal fraction of human lung macrophages. The antibody recognizes CD68, a heavily glycosylated type I transmembrane glycoprotein belonging to the lysosomal-associated membrane protein (LAMP) family. A defining characteristic of KP1 is its recognition of a fixation-resistant epitope, which allows it to be used effectively on routinely processed, paraffin-embedded tissue sections. This epitope is likely glycan-based and recognizes a molecule of approximately 110 kilodaltons in macrophage-rich human tissue. Cellular Reactivity and DistributionKP1 demonstrates broad reactivity with cells of the mononuclear phagocytic lineage, staining tissue macrophages including Kupffer cells, germinal centre macrophages, splenic macrophages, and lamina propria macrophages. The antibody also reacts with granulocyte precursors. CD68 localizes predominantly to lysosomal membranes, with a small amount present on the cell surface, and can be found in the cytoplasm of monocytes/macrophages, fibroblasts, human peripheral blood lymphocytes, neutrophil primary and mast cell granules, large granular lymphocytes, basophils, and various other cell types. Importantly, while KP1 was originally used as a pan-monocytic/macrophage marker, CD68 is not macrophage-specific, and KP1 is known to stain neutrophils and other non-macrophage-like cells. Interdigitating reticulum cells show limited or no staining, while Langerhans' cells and follicular dendritic reticulum cells remain unreactive. Clinical and Diagnostic ApplicationsKP1 has proven valuable for studying disorders of the monocyte/macrophage system, including both reactive and neoplastic states such as true histiocytic proliferations. The antibody reacts with CD68 in a wide range of healthy and disease-associated tissues, including those from patients with rheumatoid arthritis and osteoarthritis, as well as various neoplasms, tumor cell lines, and tumor-associated macrophages. In hematological malignancies, KP1 shows specific staining patterns that aid in diagnosis. It labels acute leukemias of M4 and M5 types and rare examples of malignant histiocytosis/true histiocytic sarcoma. The antibody shows strong granular cytoplasmic staining in chronic and acute myeloid leukemia and reacts with rare cases of true histiocytic neoplasia. Comparative AdvantagesWhen compared to other macrophage markers, KP1 offers distinct advantages. The PG-M1 antibody, another CD68 antibody, showed more restricted reactivity with elements of the monocyte/macrophage lineage than KP1 in routine paraffin sections. Unlike PG-M1, which detects a macrophage-restricted form of the CD68 antigen, KP1 reacts with both macrophages and myeloid cells. This broader reactivity makes KP1 particularly useful for comprehensive studies of the mononuclear phagocytic system across different tissue types and pathological conditions. Dosing regimens of clone KP1 (anti-human CD68) primarily depend on the application and mouse model; most commonly, KP1 is used for immunostaining with a fixed dilution (typically 1:200) in humanized mouse models, whereas in vivo functional or gene transfer applications may use a defined titer or dose per weight. Key regimens reported include:
Summary table:
*Note: "AAV-KP1" refers to an adeno-associated virus vector and not the anti-CD68 antibody itself. Essential context:
If searching for dosing regimens for KP1 outside immunostaining (for in vivo intervention or functional studies), current literature and commercial protocols do not indicate standard dosages. For more specialized uses, dose selection may require empirical optimization. References & Citations1. Holness CL, Simmons DL. Blood. 81(6):1607-1613. 1993.
2. Saito N, Pulford KA, Breton-Gorius J, et al. Am J Pathol. 139(5):1053-1059. 1991. 3. Saitoh O, Wang WC, Lotan R, et al. J Biol Chem. 267(8):5700-5711. 1992. 4. Pulford KA, Sipos A, Cordell JL, et al. Int Immunol. 2(10):973-980. 1990. 5. Kunisch E, Fuhrmann R, Roth A, et al. Ann Rheum Dis. 63(7):774-784. 2004. 6. Beranek JT. Ann Rheum Dis. 64(2):342-343; author reply 343-344. 2005. 7. Gottfried E, Kunz-Schughart LA, Weber A, et al. Scand J Immunol. 67(5):453-463. 2008. 8. Frafjord A, Skarshaug R, Hammarström C, et al. Scand J Immunol. 92(1):e12889. 2020. 9. Warnke RA, Pulford KA, Pallesen G, et al. Am J Pathol. 135(6):1089-1095. 1989. 10. Pulford KA, Rigney EM, Micklem KJ, et al. J Clin Pathol. 42(4):414-421. 1989. 11. Smith ME, Costa MJ, Weiss SW. Am J Surg Pathol. 15(8):757-763. 1991. 12. Micklem K, Rigney E, Cordell J, et al. Br J Haematol. 73(1):6-11. 1989. Technical ProtocolsB EM  ICC ICFC  IHC FFPE   Certificate of Analysis |
Formats Available
 Products are for research use only. Not for use in diagnostic or therapeutic procedures.
Products are for research use only. Not for use in diagnostic or therapeutic procedures.