

Anti-Human EGFR (Panitumumab) [Clone ABX-EGF]


Anti-Human EGFR (Panitumumab) [Clone ABX-EGF]
Product No.: LT620
Product No.LT620 Clone ABX-EGF Target EGFR Product Type Biosimilar Recombinant Human Monoclonal Antibody Alternate Names Epidermal growth factor receptor, ErbB1, Anti-Human EGFR, ABX-EGF 339177-26-3 Isotype Human IgG2κ Applications ELISA , FA , FC , IP , WB |
Data
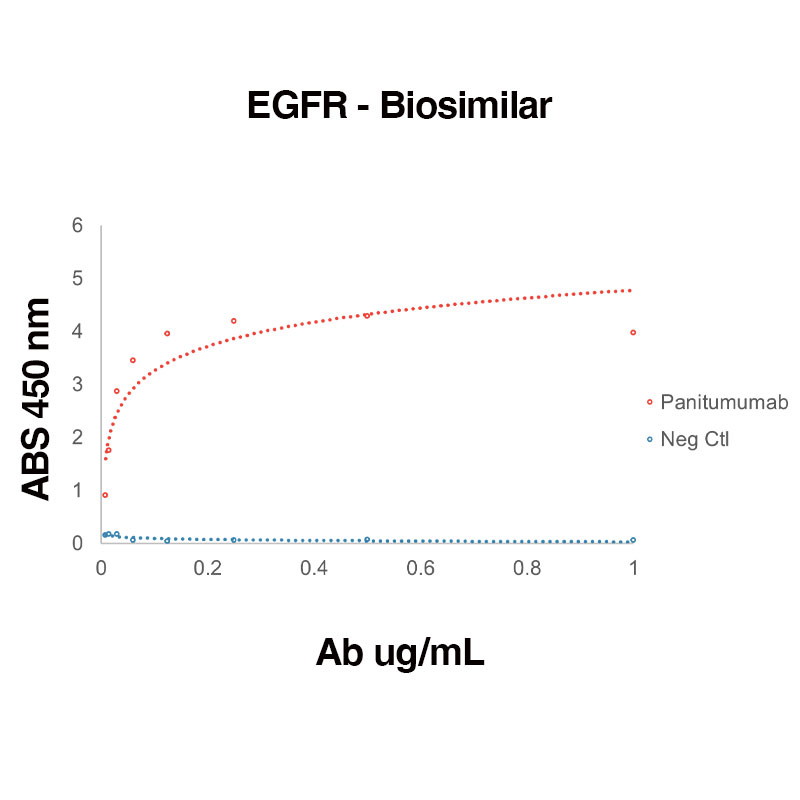 Direct binding of Human Recombinant EGFR (Leinco Prod. No.: E309) to anti-Human EGFR Panitumumab (Leinco Prod. No.: LT620)
Direct binding of Human Recombinant EGFR (Leinco Prod. No.: E309) to anti-Human EGFR Panitumumab (Leinco Prod. No.: LT620)
Binding was measured by ELISA. Recombinant Human EGFR was immobilized at 1 µg/mL. Panitumumab antibody was titrated.
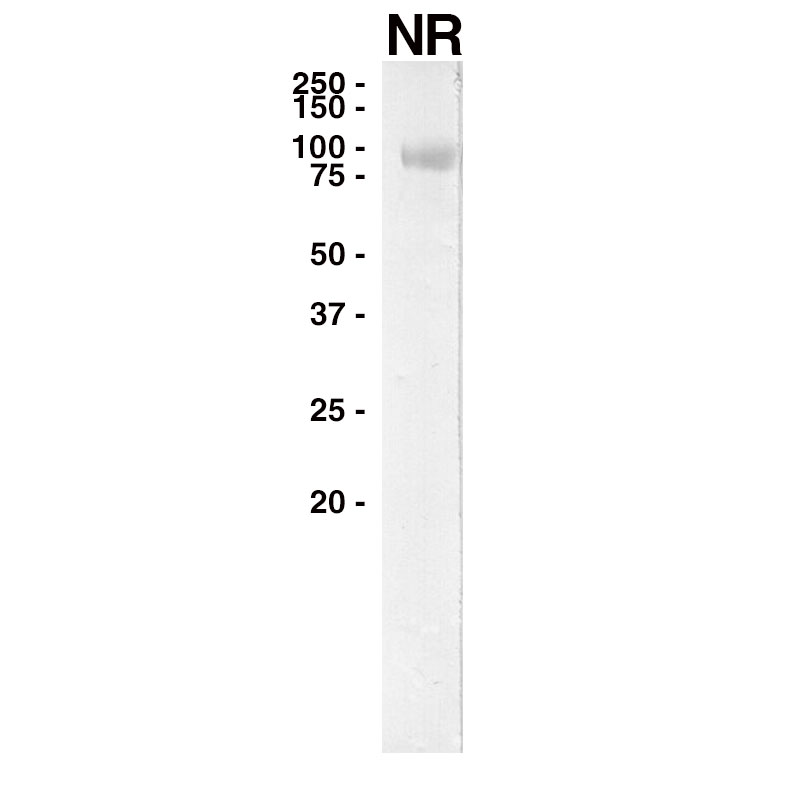 WESTERN
WESTERN
Purified recombinant human EGFR (Leinco Prod. No.: E309) was separated on SDS-PAGE under non-reducing conditions and probed with Panitumumab (Leinco Prod. No.: LT620).
Antibody DetailsProduct DetailsReactive Species Human Host Species Human Expression Host HEK-293 Cells FC Effector Activity Active Immunogen Human EGFR/ErbB1 Product Concentration ≥ 5.0 mg/ml Endotoxin Level < 1.0 EU/mg as determined by the LAL method Purity ≥95% by SDS Page ⋅ ≥95% monomer by analytical SEC Formulation This biosimilar antibody is aseptically packaged and formulated in 0.01 M phosphate buffered saline (150 mM NaCl) PBS pH 7.2 - 7.4 with no carrier protein, potassium, calcium or preservatives added. Due to inherent biochemical properties of antibodies, certain products may be prone to precipitation over time. Precipitation may be removed by aseptic centrifugation and/or filtration. State of Matter Liquid Product Preparation Recombinant biosimilar antibodies are manufactured in an animal free facility using only in vitro protein free cell culture techniques and are purified by a multi-step process including the use of protein A or G to assure extremely low levels of endotoxins, leachable protein A or aggregates. Pathogen Testing To protect mouse colonies from infection by pathogens and to assure that experimental preclinical data is not affected by such pathogens, all of Leinco’s recombinant biosimilar antibodies are tested and guaranteed to be negative for all pathogens in the IDEXX IMPACT I Mouse Profile. Storage and Handling Functional grade preclinical antibodies may be stored sterile as received at 2-8°C for up to one month. For longer term storage, aseptically aliquot in working volumes without diluting and store at ≤ -70°C. Avoid Repeated Freeze Thaw Cycles. Regulatory Status Research Use Only (RUO). Non-Therapeutic. Country of Origin USA Shipping 2-8°C Wet Ice Applications and Recommended Usage? Quality Tested by Leinco FA, ELISA, WB Additional Applications Reported In Literature ? IP, FC Each investigator should determine their own optimal working dilution for specific applications. See directions on lot specific datasheets, as information may periodically change. DescriptionDescriptionSpecificity This non-therapeutic biosimilar antibody uses the same variable region sequence as the therapeutic antibody Panitumumab. This product is for research use only. Panitumumab activity is directed against Human EGFR. Background Epidermal growth factor receptor (EGFR, also known as ErbB1 or HER-1) belongs to the receptor tyrosine kinase superfamily and is a transmembrane glycoprotein that activates various signaling pathways fundamental to cellular proliferation, differentiation, and survival1, 2. EGFR plays important roles during embryogenesis, organogenesis, and in the growth, differentiation, maintenance, and repair of adult tissues2. EGFR is also a host factor that facilitates viral entry for hepatitis B4, hepatitis C5, and gastroenteritis6 and plays a role in SARS-CoV-2 infection7, 8, 9.
Dysregulation, somatic mutation, and/or altered signaling of EGFR is associated with neurological diseases (e.g. Parkinson’s2, Alzheimer’s1, 2, and amyotrophic lateral sclerosis2) and multiple cancers (lung, glioblastoma, brain, breast, colorectal, ovarian)10. Additionally, in cancer, binding of ligands to EGFR is associated with aberrant cell proliferation, invasion, metastasis, angiogenesis, and decreased apoptosis11. As such, EGFR is the target of multiple cancer therapies, including monoclonal humanized antibodies, such as panitumumab, as well as selective small molecule inhibitors. Panitumumab was generated in a XenoMouse IgG2 strain immunized with the human cervical epidermal carcinoma cell line A43112. Panitumumab binds specifically to EGFR and inhibits the growth and survival of selected human tumor cell lines over-expressing EGFR in vitro and in vivo13. Panitumumab binds EGFR with high affinity, blocking the binding of both EGF and TGF-α, and preventing EGF-activated EGFR tyrosine autophosphorylation and downstream activation of receptor-associated kinases12. Panitumumab inhibits cell growth, tumor cell activation, in vitro tumor cell proliferation12, and metastasis13. Panitumumab also induces apoptosis and decreases proinflammatory cytokine and vascular growth factor production13. Additionally, upon binding, panitumumab causes EGFR internalization in tumor cells12. Panitumumab was approved in the United States for the treatment of some patients with EGFR-expressing metastatic colorectal cancer14, 15. Antigen Distribution EGFR is overexpressed on the cell surfaces of various tumor cell types and is also found in the plasma membranes, cytoplasm, and cell junctions of many healthy tissues, including those associated with the Skin – Epidermis development cluster of The Human Protein Atlas. EGFR is also found in the blood secretome. Ligand/Receptor Epidermal growth factor receptor PubMed NCBI Gene Bank ID UniProt.org Research Area Biosimilars . Cancer . Cell Biology . Immuno-Oncology . Immunology . Organoid Leinco Antibody AdvisorPowered by AI: AI is experimental and still learning how to provide the best assistance. It may occasionally generate incorrect or incomplete responses. Please do not rely solely on its recommendations when making purchasing decisions or designing experiments. In a pharmacokinetic (PK) bridging ELISA for measuring drug concentration in serum samples, research-grade Panitumumab biosimilars can be used as calibration standards or reference controls by following these steps: Development of the PK Assay
Use of Panitumumab Biosimilars as Calibration Standards
Application in PK Bridging Studies
In summary, research-grade Panitumumab biosimilars can be used as calibration standards in PK bridging ELISA assays if they have been bioanalytically validated against the reference product, ensuring that the assay accurately measures drug concentrations in serum samples and supports the bioequivalence assessment required for regulatory approval. The primary in vivo models where a research-grade anti-EGFR antibody is administered to study both tumor growth inhibition and to characterize tumor-infiltrating lymphocytes (TILs) are:
1. Human Tumor Xenograft Models (in Immunodeficient or Humanized Mice):
2. Syngeneic Mouse Tumor Models:
Key Application Notes:
Summary: Based on the available research literature, there appears to be limited direct evidence of researchers specifically combining panitumumab biosimilars with checkpoint inhibitors like anti-CTLA-4 or anti-LAG-3 biosimilars in immune-oncology studies. However, the existing research provides important insights into the mechanisms and potential for such combinations. Panitumumab's Mechanism of ActionPanitumumab is a fully human IgG2 monoclonal antibody that targets the epidermal growth factor receptor (EGFR) with high affinity, completely blocking ligand binding and downstream kinase cascade activation. Unlike other EGFR inhibitors, panitumumab contains no murine protein sequences, significantly reducing hypersensitivity reaction risks. The drug demonstrates sustained antitumor effects, with tumor growth inhibition lasting up to 8 months after treatment discontinuation in preclinical models. Checkpoint Inhibitor Combination MechanismsResearch has revealed distinct mechanisms of action between different checkpoint inhibitor combinations. Studies using mouse models of melanoma have shown that anti-PD-1/LAG-3 combinations require CD4 T-cells for their anticancer effects, while anti-PD-1/CTLA-4 combinations do not require CD4 T-cell presence. The anti-PD-1/LAG-3 regimen decreases regulatory T-cell activity and increases CD4 helper T-cell activity, leading to CD8 T-cell activation, whereas anti-PD-1/CTLA-4 treatment results in direct accumulation and activation of cytotoxic CD8 T-cells. Rationale for Multi-Pathway TargetingThe combination of multiple checkpoint inhibitors is based on targeting different pathways simultaneously to overcome individual therapy limitations. Anti-CTLA-4 primarily acts in lymph node compartments to restore T-cell induction and proliferation, while anti-PD-1 acts peripherally at tumor sites to prevent cytotoxic T-cell neutralization by PD-L1 expressing cells. Biomarker Considerations for PanitumumabCritical to combination strategies is understanding biomarker profiles that predict panitumumab efficacy. Research demonstrates that K-RAS wild-type patients show significantly better progression-free survival (12.3 vs 7.3 weeks) compared to those with K-RAS mutations when treated with panitumumab. Additionally, PIK3CA mutations and PTEN loss are associated with lack of objective response to panitumumab, with patients harboring these mutations showing worse clinical outcomes. Current Research GapsWhile the mechanistic rationale for combining EGFR inhibitors like panitumumab with checkpoint inhibitors exists, specific studies examining panitumumab biosimilars in conjunction with checkpoint inhibitor biosimilars in complex immune-oncology models are not well-documented in the current literature. The research primarily focuses on individual drug mechanisms and traditional combinations rather than biosimilar-specific combination strategies. Future research directions likely involve leveraging the complementary mechanisms - panitumumab's direct tumor cell targeting through EGFR inhibition combined with checkpoint inhibitors' immune system activation - to create synergistic antitumor effects while considering patient-specific biomarker profiles for optimal treatment selection. A Panitumumab biosimilar can be used as either the capture or detection reagent in a bridging ADA (Anti-Drug Antibody) ELISA to monitor a patient’s immunogenic response by detecting antibodies that patients develop against the therapeutic drug. In the bridging ADA ELISA format:
Detection is typically performed using a substrate for the enzyme label (e.g., TMB for HRP), resulting in a quantifiable color change that indicates the presence of ADAs. Key supporting details:
Summary of procedure:
Using a Panitumumab biosimilar as the capture and/or detection reagent in a bridging ADA ELISA provides a robust method for monitoring patient immune responses to the therapeutic, covering possible cross-reactivity between biosimilar and reference products. References & Citations1. Jayaswamy PK, Vijaykrishnaraj M, Patil P, et al. Ageing Res Rev. 83:101791. 2023.
2. Romano R, Bucci C. Cells. 9(8):1887. 2020. 3. Sigismund S, Avanzato D, Lanzetti L. Mol Oncol. 12(1):3-20. 2018. 4. Iwamoto M, Saso W, Sugiyama R, et al. Proc Natl Acad Sci U S A. 116(17):8487-8492. 2019. 5. Lupberger J, Zeisel MB, Xiao F, et al. Nat Med. 17(5):589-595. 2011. 6. Hu W, Zhang S, Shen Y, et al. Virology. 521:33-43. 2018. 7. Klann K, Bojkova D, Tascher G, et al. Mol Cell. 80(1):164-174.e4. 2020. 8. Xu G, Li Y, Zhang S, et al. Cell Res. 31(12):1230-1243. 2021. 9. Wang S, Qiu Z, Hou Y, et al. Cell Res. 31(2):126-140. 2021. 10. Sigismund S, Avanzato D, Lanzetti L. Mol Oncol. 12(1):3-20. 2018. 11. Garnock-Jones KP. Drugs. 76(2):283-289. 2016. 12. Yang XD, Jia XC, Corvalan JR, et al. Crit Rev Oncol Hematol. Apr;38(1):17-23. 2001. 13. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/125147s080lbl.pdf 14. Dubois EA, Cohen AF. Br J Clin Pharmacol. 68(4):482-483. 2009. 15. Saltz L, Easley C, Kirkpatrick P. Nat Rev Drug Discov. 5(12):987-988. 2006. 16. Giusti RM, Shastri KA, Cohen MH, et al. Oncologist. 12(5):577-583. 2007. Technical Protocols FA    Certificate of Analysis |
Formats Available
Prod No. | Description |
|---|---|
LT620 | |
LT625 |
 Products are for research use only. Not for use in diagnostic or therapeutic procedures.
Products are for research use only. Not for use in diagnostic or therapeutic procedures.