IL-2 is a 17.2 kD cytokine signaling protein that is the regulator of the proliferative and suppressive phases of the immune response, and stimulates growth and differentiation of B cells, NK cells, LAK cells, monocytes, and oligodendrocytes. It functions as a primary regulator of T cell homeostasis. Il-2 regulates the activities of white blood cells and plays a role in the immune system via “self” and “non-self” discrimination. IL-2 is a prime candidate in immunotherapeutics for both increasing T cell levels/function and for augmenting vaccine-elicited viral-specific T cell responses. IL-2 signal can be transduced via 3 different signaling pathways that include the JAK-STAT, PI3K/Akt/mTOR and MAPK/ERK pathways. Aldesleukin is a form of recombinant interleukin-2 for the treatment of cancers including malignant melanoma and renal cell cancer. Furthermore, there is additional therapeutic potential for IL-2 mAb use with transplants and autoimmune disease.
Protein Details
Purity
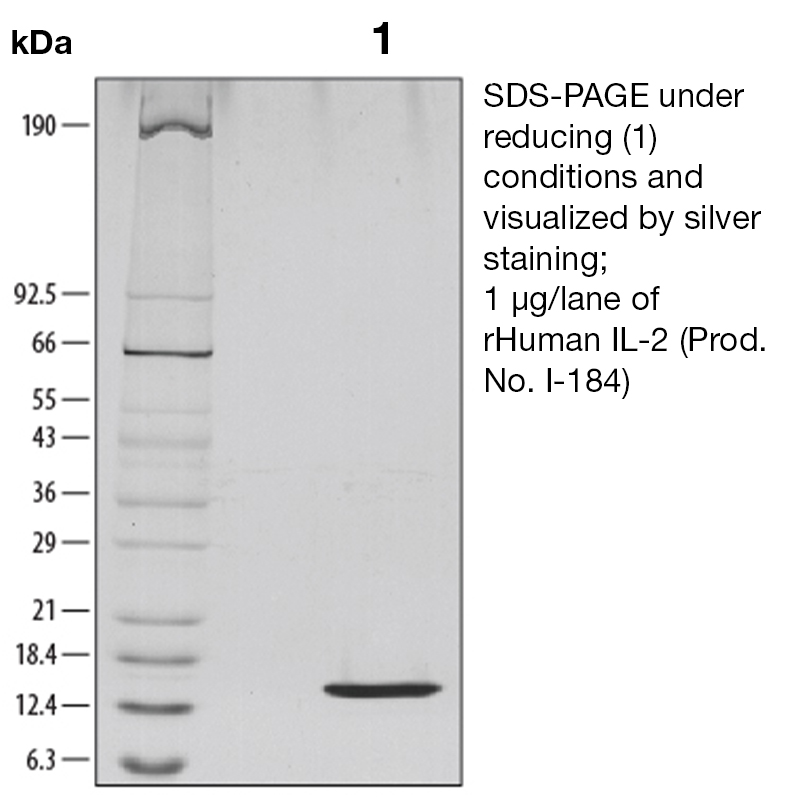
>97% by SDS-PAGE and analyzed by silver stain.
Endotoxin Level
<0.1 EU/µg as determined by the LAL method
Biological Activity
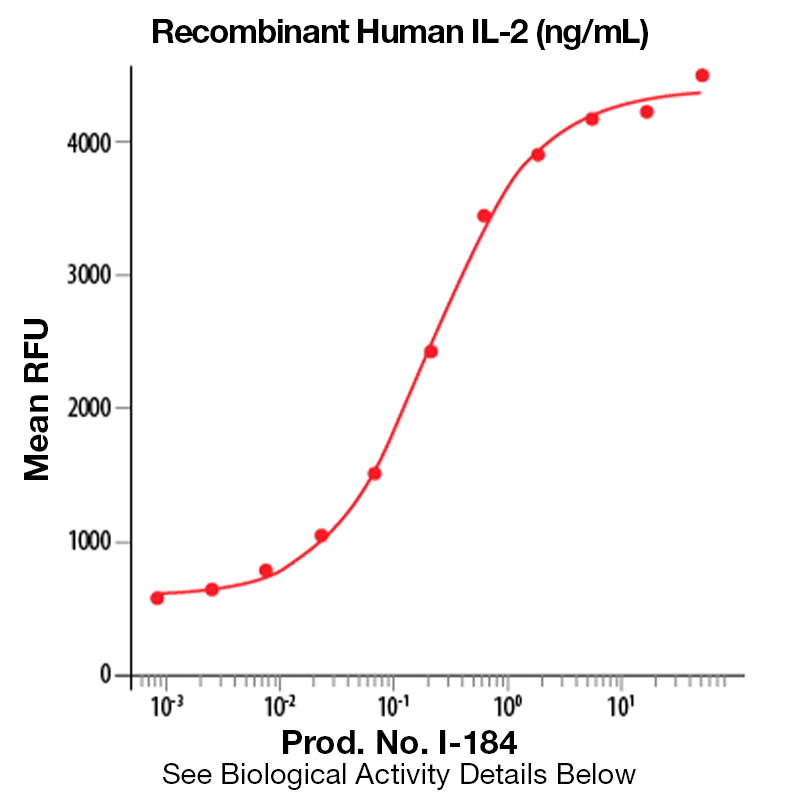
The biological activity of Human IL-2 was determined in a cell proliferation assay using an IL-2 dependent murine cytotoxic T cell line, CTLL-2 (Gearing, A.J.H. and C.B. Bird in Lymphokines and Interferons, a Practical Approach. 1987, M.J. Clemens, A.G. Morris and A.J.H. Gearing, eds., IRL Press, p. 295). The expected ED<sub>50</sub> for this effect is typically 0.25 - 0.5 ng/ml.
The predicted molecular weight of Recombinant Human IL-2 is Mr 15 kDa. However, the actual molecular weight as observed by migration on SDS-PAGE is Mr 13 kDa.
Predicted Molecular Mass
15
Formulation
This recombinant protein was lyophilized from 0.2 µm filtered solutin in 30%(v/v) Acetonitrile and 0.1%(v/v) TFA.
Storage and Stability
This lyophilized protein is stable for six to twelve months when stored desiccated at -20°C to -70°C. After aseptic reconstitution, this protein may be stored at 2°C to 8°C for one month or at -20°C to -70°C in a manual defrost freezer. Avoid Repeated Freeze Thaw Cycles. See Product Insert for exact lot specific storage instructions.
Powered by AI: AI is experimental and still learning how to provide the best assistance. It may occasionally generate incorrect or incomplete responses. Please do not rely solely on its recommendations when making purchasing decisions or designing experiments.
Recombinant Human IL-2 is widely used in research applications because it is a potent cytokine that regulates immune cell proliferation, differentiation, and function, making it essential for studies involving T cells, NK cells, B cells, and immune modulation.
Key scientific reasons to use recombinant human IL-2 in research include:
T Cell Expansion and Activation: IL-2 is critical for the proliferation and activation of CD4+ and CD8+ T cells, which is fundamental for immunological assays, adoptive cell therapies, and CAR-T cell manufacturing workflows.
NK and B Cell Stimulation: IL-2 also promotes the growth and functional activity of natural killer (NK) cells and B cells, supporting research in innate and adaptive immunity.
Regulatory T Cell Development: IL-2 is essential for the development, survival, and function of regulatory T cells (Tregs), which are crucial for immune tolerance and studies of autoimmune diseases.
Cancer Immunotherapy Research: Recombinant IL-2 has been pivotal in developing immunotherapies, especially for metastatic melanoma and renal cell carcinoma, and is used to expand tumor-infiltrating lymphocytes for adoptive cell transfer studies.
Autoimmunity and Immune Modulation: Low-dose IL-2 is being investigated for its ability to selectively expand Tregs and modulate immune responses in autoimmune and inflammatory disease models.
Reproducibility and Purity: Recombinant production ensures high purity, low endotoxin levels, and batch-to-batch consistency, which are critical for reliable experimental outcomes.
Additional considerations:
Validated Bioactivity: Recombinant IL-2 is biologically active and validated in cell-based assays, ensuring its effectiveness in experimental protocols.
Scalability and Supply: Recombinant systems allow for scalable production, supporting large-scale experiments and clinical-grade cell manufacturing.
In summary, recombinant human IL-2 is indispensable for immunological research due to its central role in immune cell biology, therapeutic development, and experimental reproducibility.
Yes, recombinant human IL-2 can be used as a standard for quantification or calibration in ELISA assays. Multiple sources confirm that recombinant human IL-2 is specifically designed and validated for this purpose. Here are the key points:
Recombinant human IL-2 is commonly used as a standard in sandwich ELISA assays for the quantitative determination of IL-2 in samples such as cell culture supernatants, serum, and plasma.
The protein is suitable for generating a standard curve, typically through serial dilutions (e.g., doubling dilutions from 2000 pg/mL down to 15 pg/mL or similar ranges depending on the kit).
The assay will recognize both natural and recombinant human IL-2, ensuring accurate quantification.
It is recommended to reconstitute the standard according to the manufacturer's instructions and to generate a fresh standard curve for each assay to ensure accuracy.
The immunoassay is often calibrated against international reference standards (e.g., NIBSC 86/504) to ensure consistency and comparability across different laboratories and kits.
In summary, recombinant human IL-2 is an appropriate and widely used standard for calibrating and quantifying IL-2 levels in ELISA assays.
Recombinant Human IL-2 has been validated for a broad range of applications in published research, primarily in immunology, cell therapy, and cancer immunotherapy.
Key validated applications include:
Immune cell activation and proliferation: IL-2 is widely used to activate and expand T cells (both CD4⁺ and CD8⁺), regulatory T cells (Tregs), and natural killer (NK) cells in vitro and in vivo.
Cell culture and expansion protocols: Recombinant IL-2 is a standard supplement for the expansion of T cells and NK cells in cell culture, including protocols for adoptive cell therapy and CAR T cell manufacturing.
Cancer immunotherapy: High-dose recombinant IL-2 is FDA-approved for metastatic melanoma and renal cell carcinoma, where it boosts anti-tumor immune responses. It is also used in combination with immune checkpoint inhibitors and cancer vaccines.
Autoimmune disease research: Low-dose IL-2 is being investigated for selective expansion of Tregs to restore immune balance in conditions such as lupus and type 1 diabetes.
Transplantation tolerance: Modified forms of recombinant IL-2 have been validated for expanding Tregs to promote tolerance and prolong allograft survival in transplantation models.
Bioassays and functional assays: IL-2 is used as a positive control and stimulant in various immunological bioassays, including cytokine detection and quantification.
Hematopoietic stem and progenitor cell research: IL-2 supports the expansion and maintenance of certain stem and progenitor cell populations.
Chronic infection models: IL-2 has been studied for enhancing immune cell recovery and function in chronic infections such as HIV and hepatitis C.
Additional validated uses:
Screening and release assays for cell therapy products.
Differentiation studies for immune cell subsets.
Combination protocols with other cytokines (e.g., IL-15) to increase cell viability and proliferation.
These applications are supported by extensive published research and clinical studies, demonstrating recombinant human IL-2’s central role in immunological assays, cell therapy development, and translational medicine.
To reconstitute and prepare Recombinant Human IL-2 protein for cell culture experiments, dissolve the lyophilized protein in sterile 100 mM acetic acid or sterile distilled water to a concentration of at least 100 μg/mL, optionally including 0.1% carrier protein (such as human or bovine serum albumin) to enhance stability.
Step-by-step protocol:
Preparation:
Briefly centrifuge the vial to collect the powder at the bottom before opening.
Perform all steps under aseptic conditions in a biosafety cabinet.
Reconstitution:
Add sterile 100 mM acetic acid (preferred for maximum solubility and activity) or sterile distilled/deionized water to achieve a final concentration of 100 μg/mL or higher.
If using water, use the solution within 24 hours and store at 2–8 °C.
For improved stability, add at least 0.1% carrier protein (e.g., human or bovine serum albumin) to the reconstitution buffer.
Gently swirl or tap the vial to dissolve; do not vortex, as vigorous agitation may reduce biological activity.
Aliquoting and Storage:
Once fully dissolved, aliquot the solution into working volumes to avoid repeated freeze-thaw cycles.
Store aliquots at ≤ –20 °C for long-term storage. Avoid frost-free freezers.
For short-term use (up to 1 week), store at 2–8 °C.
Dilution for Cell Culture:
Make further dilutions in cell culture medium or buffer containing serum or 0.1% BSA/HSA to minimize protein loss due to adsorption.
The optimal working concentration depends on your specific assay and cell type; titrate as needed.
Additional notes:
If using a carrier-free formulation, reconstitute in 100 mM acetic acid only.
Some protocols recommend reconstitution in 10 mM HCl at 0.1 mg/mL as an alternative.
Avoid filtering the reconstituted IL-2 unless absolutely necessary, as the protein is typically provided sterile and filtration may cause loss of material.
Summary of key points:
Reconstitution buffer: 100 mM acetic acid (preferred) or sterile water.
Concentration: ≥100 μg/mL.
Carrier protein: 0.1% BSA or HSA recommended for stability.
Mixing: Gentle swirling, no vortexing.
Storage: Aliquot and freeze at ≤ –20 °C; short-term at 2–8 °C.
Dilution: Use cell culture medium with serum or BSA/HSA.
These steps will ensure that your recombinant human IL-2 is optimally prepared for cell culture applications.
References & Citations
1. Schachter, J. et al. (2009) Cytotherapy11: 206 2. Sodora, DL. et al. (2009) Curr HIV Res.7: 83 3. Alcocer-Varela, J. et al. (2009) Autoimmun Rev. 9(1):34-9.




 Products are for research use only. Not for use in diagnostic or therapeutic procedures.
Products are for research use only. Not for use in diagnostic or therapeutic procedures.