This monoclonal antibody is aseptically packaged and formulated in 0.01 M phosphate buffered saline (150 mM NaCl) PBS pH 7.2 - 7.4 with no carrier protein, potassium, calcium or preservatives added. Due to inherent biochemical properties of antibodies, certain products may be prone to precipitation over time. Precipitation may be removed by aseptic centrifugation and/or filtration.
Product Preparation
Functional grade preclinical antibodies are manufactured in an animal free facility using in vitro cell culture techniques and are purified by a multi-step process including the use of protein A or G to assure extremely low levels of endotoxins, leachable protein A or aggregates.
Storage and Handling
Functional grade preclinical antibodies may be stored sterile as received at 2-8°C for up to one month. For longer term storage, aseptically aliquot in working volumes without diluting and store at ≤ -70°C. Avoid Repeated Freeze Thaw Cycles.
Applications and Recommended Usage? Quality Tested by Leinco
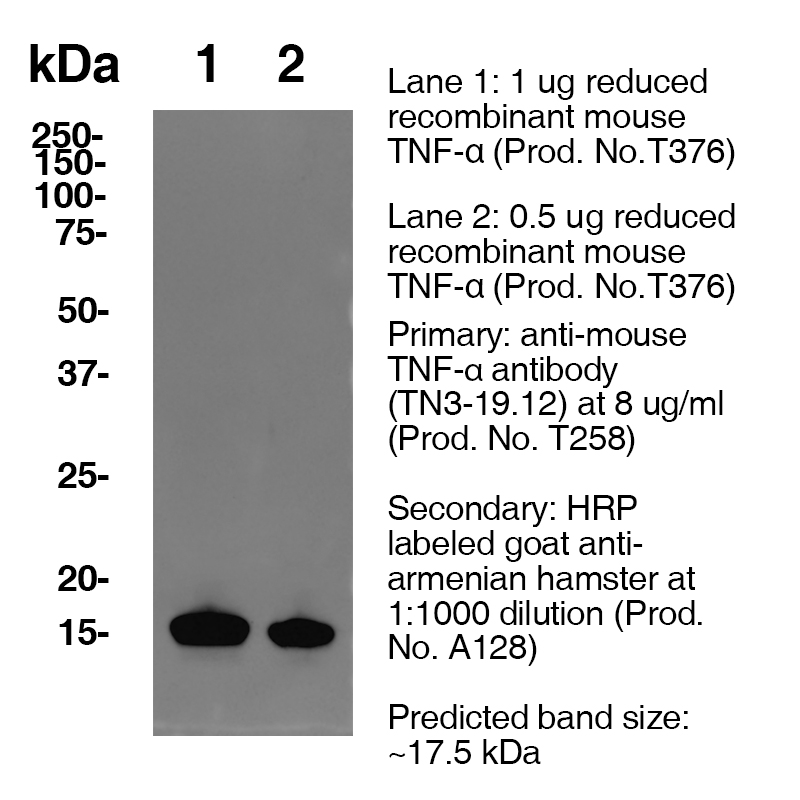
ELISA: Each lot of this antibody is quality control tested by ELISA assay. For use of this antibody as a capture, a concentration range of 2 - 6 µg/ml is recommended. To obtain a linear standard curve, serial dilutions of mouse TNF-α recombinant protein ranging from 500 to 4 pg/ml are recommended for each ELISA plate. It is recommended that the reagent be titrated for optimal performance for each application.
Additional Reported Applications For Relevant Conjugates ?
N: Clone TN3-19.12 has been shown to neutralize murine TNFα WB IP FC
Each investigator should determine their own optimal working dilution for specific applications. See directions on lot specific datasheets, as information may periodically change.
Description
Description
Specificity
Armenian Hamster Anti-Mouse TNFa (Clone TN3-19.12 ) recognizes Mouse TNFa. This monoclonal antibody was purified using multi-step affinity chromatography methods such as Protein A or G depending on the species and isotype.
Background
The tumor necrosis factor (TNF-alpha) is a multifaceted polypeptide cytokine known as a mediator of inflammation and immunity.1 It may mediate some of the significant changes in cellular homeostasis which accompany the invasion of the mammalian host by viruses, bacteria, and parasites.2 TNF-α is an acute phase protein which initiates a cascade of cytokines and increases vascular permeability, thereby recruiting macrophage and neutrophils to a site of infection. TNF-α secreted by the macrophage causes blood clotting which serves to contain the infection. TNF-α has been detected in synovial fluid of patients with rheumatoid arthritis. Clone TN3-19.12 antibody can neutralize the bioactivity of natural or recombinant TNF-α
Antigen Distribution
Activated monocytes, neutrophils, macrophages, T cells, B cells, NK cells, LAK cells
Powered by AI: AI is experimental and still learning how to provide the best assistance. It may occasionally generate incorrect or incomplete responses. Please do not rely solely on its recommendations when making purchasing decisions or designing experiments.
Clone TN3-19.12 is most commonly used in vivo in mice to neutralize endogenous TNF-alpha (tumor necrosis factor-alpha), allowing researchers to study the role of TNF-alpha in immune responses, inflammation, and various disease models.
Key in vivo applications include:
TNF-alpha neutralization studies: TN3-19.12 is injected into mice to block TNF-alpha activity, enabling the investigation of TNF-mediated pathologies such as autoimmune diseases, infections, and models of sepsis or endotoxin shock. This has been shown to protect mice from lethal endotoxin shock and to block detectable TNF in circulation following LPS challenge.
Cytokine neutralization in disease modeling: The antibody is utilized to assess TNF-alpha’s contribution in models of arthritis, infection, neuroinflammation, and cancer, among others.
Cytokine measurement facilitation: As a component in the in vivo cytokine capture assay (IVCCA), TN3-19.12 is administered to bind circulating TNF-alpha, increasing its half-life in serum and enhancing assay sensitivity for cytokine quantification. This is particularly valuable when analyzing cytokine profiles during immune responses.
ELISA and flow cytometry: The clone is used both as a capture antibody in ELISA for sensitive detection of TNF-alpha in mouse serum, and for intracellular cytokine staining and analysis by flow cytometry.
Important features of TN3-19.12 include:
Cross-reactivity: It can also neutralize mouse TNF-beta (lymphotoxin) to some extent.
Specificity: While primarily targeting TNF-alpha, the antibody binds both recombinant and natural (endogenous) cytokine forms.
Safety and dosing: Typical in vivo dosing is approximately 250 µg per mouse for neutralization studies, but optimal concentration should be empirically determined for each model.
In summary, TN3-19.12 is a standard tool for in vivo functional blockade of TNF-alpha in mice, supporting disease pathogenesis studies, cytokine quantification, and mechanistic dissection of TNF-driven immune responses.
The antibody TN3-19.12 is most frequently used in combination with the following types of antibodies or proteins in the literature:
Biotinylated or fluorochrome-conjugated anti-TNFα detection antibodies (such as Poly5160 or BioLegend Poly5160) are widely used as secondary detection reagents in ELISA, ELISPOT, and flow cytometry with TN3-19.12 as the capture antibody.
Isotype controls corresponding to the Armenian Hamster IgG isotype are standard for controlling specificity in flow cytometry and functional assays.
Recombinant mouse or rat TNFα proteins are commonly included as assay standards or positive controls in ELISAs or neutralization assays.
Companion polyclonal detection antibodies (e.g., biotinylated rabbit polyclonal anti-TNFα) are typical in sandwich ELISAs, paired with TN3-19.12 for capture.
Additional examples from published protocols include:
Alternative ELISA/ELISPOT clones: Clone 1F3F3D4 is often recommended as an alternative for ELISPOT capture.
Functional assay partner antibodies: TN3-19.12 can be paired with other cytokine-neutralizing or phenotyping antibodies in multiplex experiments to define cell subsets or cytokine interactions, such as anti-IFNγ or anti-IL-6, though specifics depend on the experimental context.
Blocking and specificity controls: Unconjugated, neutralizing TN3-19.12 is sometimes used as a blocking antibody to confirm staining specificity with conjugated forms of the antibody.
For flow cytometry: TN3-19.12 (intracellular stain, often fluorochrome-conjugated) + isotype control or blocking with unconjugated TN3-19.12.
In neutralization or in vivo experiments: TN3-19.12 paired with isotype control or appropriate detection antibody to assess functional blockade.
These combinations enable sensitive, specific detection and quantification of mouse or rat TNFα in a range of experimental settings.
Clone TN3-19.12 is a monoclonal antibody widely cited in scientific literature for its ability to effectively neutralize murine tumor necrosis factor-alpha (TNF-α) and show cross-reactivity with TNF-beta (lymphotoxin).
Key findings from its scientific citations include:
Complete Neutralization of TNF-α: TN3-19.12 can inhibit 100% of the lytic activity of both recombinant and natural murine TNF-α at specific concentrations. This neutralizing capacity extends to TNF present in various biological samples, including those produced by activated T cell clones and hybridomas.
Cross-Reactivity with TNF-β (Lymphotoxin): The antibody recognizes both TNF-α and a higher molecular weight glycosylated form consistent with TNF-β. This was established through Western blot analysis, indicating broad specificity for TNF cytokines.
In Vivo Protection: Administration of TN3-19.12 in mice challenged with endotoxin (LPS) blocked the detection of TNF in serum and protected the animals from lethal endotoxin shock, demonstrating its therapeutic potential in models of inflammation and septic shock.
Utility in Cytokine Detection Assays: TN3-19.12 is used in ELISA and in vivo cytokine capture assays (IVCCA), significantly increasing the sensitivity of cytokine detection by extending their in vivo half-life, allowing for precise measurement of TNF levels in serum.
Applications in Flow Cytometry and Staining: Conjugated forms of TN3-19.12 are recommended for intracellular staining and flow cytometric analysis of TNF-α production in immune cells.
Species Reactivity: While primarily reactive with mouse TNF-α, the antibody also reacts with rat and rabbit TNF-α as noted in numerous product citations, broadening its utility in preclinical research across species.
Research on Disease Models: TN3-19.12 has been instrumental in dissecting the role of TNF-α in various disease contexts, including inflammatory and autoimmune diseases, by enabling functional neutralization experiments.
Antigen Distribution: TNF-α detected by TN3-19.12 is expressed on a range of immune cells such as activated monocytes, neutrophils, macrophages, T cells, B cells, NK cells, and LAK cells, reflecting its central role in immune regulation.
Cited in Numerous Studies: The antibody appears in foundational studies of TNF biology, disease mechanisms, and immunological assays, including work by Sheehan et al. (J. Immunol. 1989), Finkelman et al. (Curr. Prot. Immunol. 2003), and others.
In summary, clone TN3-19.12 is a crucial reagent for neutralizing murine TNF-α/β, investigating TNF's role in immunity and inflammation, and enabling sensitive detection of TNF in laboratory animals, with broad validation across multiple studies.
Dosing regimens of clone TN3-19.12, an Armenian hamster monoclonal antibody targeting mouse TNF-α, vary significantly depending on the mouse disease model, route of administration, experimental purpose, and expected duration of TNF blockade.
Key dosing regimens across different mouse models:
General dosing range:
Typical single doses range from 250 µg/mouse (intraperitoneal) to 20–30 mg/kg (intravenous or intraperitoneal) for acute interventions in inflammatory or infectious models.
TRUC colitis model:
15 mg/kg i.p., once weekly for 4 weeks.
NOD diabetes model:
20 μg/g (i.e., 20 mg/kg) or 100 µg/injection, administered i.p. every other day for 21–24 days.
Acute endotoxemia or sepsis (LPS challenge):
Single dose prior to LPS administration; specific mass not consistently cited, but protection from endotoxin shock confirmed.
DSS colitis/other chronic models:
Comparable regimens to above, usually 10–15 mg/kg i.p. every 2–7 days, depending on study duration.
Model/Indication
TN3-19.12 Dose
Route
Frequency
Source
General acute inflammation
250 µg/mouse
i.p.
single
General acute inflammation
25–30 mg/kg
i.v./i.p.
acute (single)
TRUC colitis
15 mg/kg
i.p.
weekly ×4
NOD diabetes
20 μg/g or 100 µg/inj
i.p.
every other day ×21–24 days
DSS colitis, TNFα neutralization (for comparison, using infliximab)
10 mg/kg
i.p.
alternate days (×4/7 days)
Supporting context and details:
Route and frequency:
Most published regimens use intraperitoneal injection (i.p.), but intravenous (i.v.) dose is sometimes preferred for faster systemic distribution.
Frequency ranges from single doses for acute studies (e.g., LPS/endotoxin challenge) to multiple weekly or every-other-day injections for chronic or autoimmune models.
Neutralization efficacy:
TN3-19.12 effectively neutralizes both murine TNF-α and TNF-β (lymphotoxin, LT) in vivo and provides protection in inflammatory models such as LPS-induced endotoxemia.
Formulation and preparation:
Endotoxin-free preparations are crucial for in vivo work (e.g., Ultra-LEAF™ or similar preparations).
Variability factors:
Model-specific disease severity, TNF dynamics, and experimental duration require titration of optimal antibody dose.
Sponsors and antibody suppliers recommend pilot titrations for each new study or mutant mouse line due to variability in TNF production and sensitivity.
Summary: Typical dosing of TN3-19.12 in mice ranges between 250 µg/mouse i.p. to 30 mg/kg i.v./i.p., given acutely or repeated at set intervals, with specific regimen tailored to disease model and study design. Individual protocols must be optimized according to experimental needs.
References & Citations
1.) El-Harith el-HA et al. (2004) Saudi Med J.25: 135
2.) Adolf GR et al. (1990) Infec Immun.58: 3996
3.) Czepielewski, R. et al. (2021) Immunity54(12):2795-2811.e9 Journal Link







 Products are for research use only. Not for use in diagnostic or therapeutic procedures.
Products are for research use only. Not for use in diagnostic or therapeutic procedures.